Effects of Tooth Loss
The Physical & Psychological Effects of Tooth Loss
The Dental Health in America is Being Affected By Many Oral Health Factors Including:
- Poor Performance Of Removable Replacement Teeth
- Consequences Of Tooth Loss
- A Related Decrease in Health
- The Psychological Aspects Of Tooth Loss
From the initial consultation
to post-procedure care,
we are here to support you
every step of the way.

The goal of modern dentistry is to restore the patients mouth to normal function, comfort, esthetics, speech and health, regardless of the disease, injury, or atrophy present within the oral environment. However, the more teeth a patient is missing, the more difficult this goal becomes with traditional dentistry. As a result of continued implant research and the advances in implant techniques, predictable success is now a reality for the rehabilitation of many challenging patient situations. As our population ages this success becomes critically important in order to preserve the health of the population.
Our team is ready to help you achieve the smile you’ve always dreamed of.
Life expectancy has increased significantly past the age of retirement. In 1965, the average life span was 65 years, whereas in 1990 it was 78 years. A person 65 years old, can now expect to live 16.7 more years, and one 80 years old can expect to live more than 8 more years. This increased life expectancy has led to increased tooth loss. Currently, 26% of all Americans over the age of 65 have either lost one full arch or have lost all of their teeth. Social pleasures, including dining and dating, are diminished when the teeth are lost.
Almost 30% of the employed or retired adult US population is either missing all their teeth, all their upper teeth, one entire posterior segment (a full quarter of the mouth) or has all of their back teeth missing. A study by CW Douglas published in J. Pros. Dent. (2002, 87, 5-8), stated that:


Our goal is to restore normal function, comfort, esthetics, speech, and health to our patients when they experience tooth loss regardless of disease or injury to the oral cavity. A beautiful and functioning smile can be yours when you come see us.
- In the year 2000 there were 35.4 million denture wearers – that is approximately 17% of the population of the United States.
- The number will increase to 37.9 million by 2020
- 56.5 million dentures were made in the year 2000
- The number will increase to 61 million by 2020
In the past, dentistry for the elderly has consisted of inexpensive treatments emphasizing non-surgical approaches. Conditions of tooth loss were treated with removable replacement teeth, called full or partial dentures. Today, the full scope of dental services for elderly patients is becoming increasingly important to both the public and the profession, because of the increasing age of our society. Alternative treatment designs, which include methods to reconstruct teeth on top of dental implants and that are not removable, should be presented to almost every patient. Only when all treatment options are discussed can a persons desires related to the benefit of modern dentistry be truly appreciated.
Eventually, the need for additional retention, support, and stability, or the desire to eliminate a removable denture, are common indications for more effective and permanent solutions, such as dental implants. Dental implants, which are man-made tooth root replacements, are also increasingly used to replace a missing single tooth. Like natural tooth roots, they can be used to support permanent types of tooth replacements, or act as anchors for a removable prosthesis to replace teeth (i.e. dentures). Today, this represents the most conservative and most predictable long-term option. Traditional dentistry most often replaces the missing single tooth with a fixed bridge. This is accomplished by grinding away sound tooth structure, and crowning (capping) two or more teeth on each side of the missing tooth and joins them together with the artificial or dummy tooth. This approach increases the risk of decay of the crowned teeth, increases the risk of root canal therapy, and makes oral hygiene difficult to impossible, which in turn increases bacterial plaque retention (the cause of decay and gum disease).
We are committed to delivering
Excellence in Dental Care


Trust our expert team to
help you achieve a smile
that reflects your true self
Excellence and Expertise


With dental implants, you can restore your smile, regain your confidence, and enjoy all the benefits of having strong, healthy teeth.
Today’s technology can replace the tooth with a dental implant, which may replace a single tooth or a whole mouth of teeth, without crowning any teeth. One of the major benefits is that the remaining teeth are easier to clean and less likely to decay, and/or need root canal therapy. The average dental implant has a better long-term survival rate than the average bridge. The average bridge gets replaced every 8 to 10 years.
Consequences of Tooth Loss
Effect on the Jaw Bone
The bone in the body acts very similar to a muscle. When muscles are exercised, they grow strong and larger. When bone is exercised or stimulated, it also becomes stronger. For example, when an arm is broken and placed in a cast for six weeks, you can see the arm is smaller after this time frame, since the muscles have started to shrink or atrophy. In addition, if you evaluate the bone protected by the cast, it also becomes less dense and weaker in this period. Similarly, the bone of the jaw can only be stimulated by a tooth or by an implant. The connections between a tooth, or an implant, create and preserve the size and shape of the bone. Bone needs the stimulation of the tooth roots to maintain its form, density, and strength. Scientific studies have proven that the normal chewing forces that are transmitted from the teeth to the bone of the jaw are what preserves the bone and keeps it strong.

In this photo, it is easy to see how the ridge has collapsed. The tooth was removed and, without stimulation or grafting, the bone and gum have disappeared.
This close relationship between the tooth and the bone continues throughout life. When a tooth is lost, the lack of stimulation to the surrounding bone results in a decrease in the density and dimensions of the bone. This means that there is a loss of width and height of the bone. In a 25-year study of patients with no teeth, x-rays demonstrated continued bone loss of the jaws during this entire time span. Therefore, a tooth is necessary both to the development of the bone around the tooth, and is also necessary for the stimulation of this bone to maintain its strength, density and shape. The loss of all of the teeth slowly, but eventually, leads to jaws with almost complete bone loss. A lower jaw, which starts out two inches in height, can be reduced to less than one-quarter of an inch by atrophy over time. That is one reason why modern dentistry is so excited about using dental implants to replace missing teeth.
Patients wearing dentures don’t realize they are losing bone. Over time, the poor fit and function of the denture is often thought to be due to its age, weight loss by the patient, or wear of the dentures teeth. The rate and amount of bone loss may be influenced by gender (females lose more bone), hormones (lack of estrogen causes more bone loss), metabolism, medications, parafunction (grinding the teeth) and poorly fitting dentures. Despite this, almost 40% of denture wearers have been wearing the same denture for more than 10 years. Although the fact that wearing dentures day and night places greater forces on the bone and gum, and accelerates bone loss, 80% of dentures are worn both day and night.
Consider the following: The issue of bone loss after tooth loss has been ignored in the past by traditional dentistry. This is so because dentistry had no treatment to stop or prevent the process of bone loss and its consequences. As a result, doctors had to ignore the inevitable bone loss after tooth extraction. Today, the profession knows about bone loss, and that implants can stop bone loss because they stimulate the bone, similar to the way the tooth did prior to its loss.
Jaws with bone loss are associated with problems, which often impair the predictable results of traditional dentures. The loss of bone first results in decreased bone width. There is a 25% decrease in width of bone during the first year after tooth loss and an overall _-inch decrease in height during the first year following extractions of several teeth. The remaining narrow bone often causes discomfort when the thin overlying gum tissues are loaded under a complete or partial denture. In the lower jaw, the continued bone loss eventually results in prominent bony projections covered by thin, movable, unattached gum tissue. As the remaining bone on the front of the jaw continues to disappear, the bony projection under the tongue rises to sit on the top of ridge. This results in pain, as the denture sits atop the sharp bony projection. In addition, there is little to prevent the denture from moving forward against the lower lip during function or speech. The problems are further compounded by the upward movement of the back of the denture during contraction of the muscles during speech and function. The resulting incline (slope) of the now deformed lower jaw compared with that of the upper jaw also creates instability and movement of the lower denture.
Loss of bone in the upper and lower jaw is not limited to the bone around the teeth; portions of the skeletal bone also may be lost especially in the back parts of the lower jaw where the patient may lose more than 80% of the bone. The nerves of the lower jaw which were surrounded by and protected by bone eventually become exposed and sit on the top of the ridge directly under the denture. As a result, acute pain and/or temporary to permanent loss of sensation or feeling of the areas supplied by the nerve is possible. The bone loss in the upper jaw may cause pain and an increase in upper denture movement during eating. The forces from eating with an ill-fitting denture are transferred directly to the surface only and not the internal structure of the bone since there are no roots. Therefore, these forces do not stimulate and maintain the bone, but instead actually decrease blood supply and increased the rate of the bone loss. Chewing forces generated by short facial types can be 3 or 4 times that of long facial types. These patients are at even greater risk to develop severe bone loss.
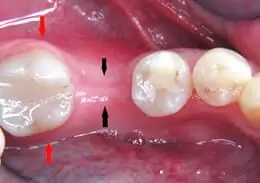
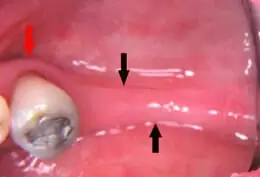
This photo shows a lower ridge that has lost 60% of its width following an extraction and normal healing. The black arrows indicate where bone is located (compare the width to the adjacent molar). The red arrows indicate the normal width that should be there.
Many of these conditions that have been described for patients without any teeth also exist for patients where only back teeth are missing and they are wearing a removable partial denture. The above problems focus on the damage to the bone. The remaining natural teeth are also subjected to substantial damage. The teeth must support the partial denture by connections called clasps. The clasps grab onto the teeth, and by design, transfer lateral or sideward forces to the teeth, which weaken them and cause tooth loss. Since these teeth often become compromised by loss of bone due to these forces, many partial dentures are then designed to minimize the forces applied upon these teeth. The net result is an increase in movement of the removable denture, and greater pressures on the soft gum tissue over the bone. This results in more bone loss. These conditions can protect the remaining teeth, but then accelerate the bone loss in the regions without teeth.

Throughout this process, your comfort and understanding are our top priorities.
Effect on Soft Tissue
As bone continues to lose width and height, the gum tissues gradually decrease. A very thin gum usually lies over the advanced bone loss of the lower jaw. The gum is prone to sore spots caused by the overlaying denture. In addition, unfavorable high muscle attachments and loose tissue often complicates the situation.
The tongue of the patient with no teeth often enlarges to accommodate the increase in space formerly occupied by teeth. At the same time, the tongue is used to limit the movements of the removable denture, and takes a more active role in the chewing of food. As a result, the removable denture decreases in stability. The decrease in muscular control, often associated with aging, further compounds the problems of traditional removable dentures. The ability to wear a denture successfully may be largely a learned, skilled performance. The aged patient who recently loses their teeth may lack the motor skills needed to accommodate to the new conditions. This often results in food that is not adequately chewed, resulting in digestion and nutrition problems. (See Health Effects of Tooth Loss below)
Never again suffer from the use of dentures, or the pain and embarrassment of missing teeth. Ever!

Effects of Bone Loss on Facial Appearance
Facial changes naturally occur in relation to the aging process. When the teeth are lost, this process is grossly accelerated with more rapid facial aging. The loss of teeth can add 10 or more years to a person’s face. A decrease in face height occurs as a result of the collapse of bone height when teeth are lost. This results in several facial changes. The decrease in the angle next to the lips and deepening of vertical lines on the lips create a harsher appearance. As the vertical bone loss progressively and rapidly increases, the bite relationship deteriorates. As a result, the chin rotates forward and gives a poorer facial appearance. These conditions result in a decrease in the angle at the corner of the lips, and the patient appears unhappy when the mouth is at rest. Short facial types have higher bite forces, greater bone loss and more facial changes with tooth loss, compared to others. A thinning of the upper lip results from the poor lip support provided by the denture. And, there is a loss of tonicity of the muscles. Women often use one of two techniques to hide this cosmetically undesirable appearance: either no lipstick and minimum make-up, so that little attention is brought to this area of the face or lipstick is drawn over the border of the lips to give the appearance of fuller lips.
The upper lip naturally becomes longer with age as a result of gravity and loss of muscle tone. The loss of muscle tone is accelerated in a patient with no teeth hence the lengthening of the lip occurs at a younger age. Men often grow a moustache to minimize this effect. This has a tendency to age the smile, because the younger the patient, the more the teeth show in relation to the upper lip at rest or when smiling. A deepening of the groove next to the nose and an increase in the depth of other vertical lines are made worse by the bone loss in the upper front jaw. This usually is accompanied by an increase in the angle under the nose. This can make the nose appear larger. The attachments of the muscles to the jaw also are affected by bone loss. The tissue sags along the lower jaw with bone loss, producing jowls or a witch’s chin. This effect is additive because of the loss of muscle tone along with the loss of teeth.
This photo shows just how much bone can be lost and how thin a ridge can become before it disappears completely.
Patients are unaware that these bone, gum and facial changes are due to the loss of teeth. Instead, they blame these problems on aging, weight loss, or the dentist for making a poor denture.
Health Effects of Tooth Loss
A study of 367 denture wearers (158 men and 209 women) found that 47% exhibited a low chewing performance. Lower intakes of fruit and vegetables and vitamin A were also noted in this group. These patients took significantly more drugs (37%) compared to those with superior chewing ability (20%), and 28% were taking medications for stomach or intestinal disorders. The reduced consumption of high fiber foods could therefore induce stomach or intestinal problems in patients without teeth with deficient chewing performance. In addition, as the coarser food is chewed it may impair proper digestive and nutrient extraction functions. The literature provides several reports that suggest that compromised dental function results in poor swallowing and chewing performance which in turn may negatively affect overall health and favor illness, debilitation, and shortened life expectancy.
Several reports in the literature correlate patients health and life span to their dental health. After conventional risk factors for stroke and heart attacks were accounted for, there was a significant relationship between dental disease and heart or blood vessel disease, still the major cause of death. It is legitimate to believe that restoring the mouth of patients to a more normal function may indeed enhance the quality and length of life.

CHECK OUR
Patient reviews
“Very knowledgeable and friendly staff…”
Psychological Aspects of Tooth Loss
The psychological effects of total tooth loss are complex and varied, and range from very minimal to a state of anxiety. Although complete dentures are able to satisfy the appearance needs of many patients, there are many who feel their social life is significantly affected. They are concerned with kissing and romantic situations, especially if a new relationship is unaware of their oral handicap. A past dental health survey indicates that only 80% of the population without teeth is able to wear both upper and lower dentures all of the time. Some patients wear only one of the dentures, usually the upper; others are able to wear their dentures only for short periods. In addition, approximately 7% of denture wearers are not able to wear them at all, and become dental cripples or oral invalids. They rarely leave their home environment, and when they feel forced to venture out, the thought of meeting and talking to people while not wearing teeth is unsettling.
Misch and Misch performed a study of 104 patients missing all of their teeth and seeking treatment. A total of 88% of the patients claimed difficulty with speech, with 25% of that population reporting very difficult problems. It is easy to correlate the reported increase in concern relative to social activities. Movement of the lower denture was reported by 62.5% of these patients. The upper denture stayed in place at almost the same percentage. Lower jaw discomfort was listed with equal frequency as movement (63.5%), and 16.5% stated they never wear the lower denture. The psychological effects of the inability to eat in public can be correlated to these findings. In comparison, the upper denture was uncomfortable half as often (32.6%), and only 0.9% of patients were seldom able to wear the denture. Function was the fourth problem reported. Half of the patients avoided many foods, and 17% claimed they were able to chew more effectively without the denture.
The psychological needs of the patient without teeth can be expressed in many forms. For example, in 1982 more than 5 million Americans used denture adhesives. A recent report showed that in the United States more than $147 million is spent each year on denture adhesives, representing 45 million units sold. The patient is willing to accept the unpleasant taste, need for recurrent application, inconsistent denture fit, embarrassing circumstances, and continued expense for the sole benefit of increased retention of the denture.
In contrast, 80% of the patients treated with implant-supported prostheses judged their overall psychological health improved compared with their previous state wearing traditional, removable dentures, and perceived the implant-supported prosthesis (denture) as an integral part of their body. Clearly, the lack of retention and psychological risk of embarrassment in the denture wearer is a concern the dental profession must address.
Decreased Performance of Removable Dentures

The difference in maximum bite forces recorded in a person with natural teeth and one who is completely without teeth is dramatic. In the first molar region of a person with teeth, the average force has been measured at 150 to 250 pounds per square inch (psi). A patient who grinds or clenches the teeth may exert a force that approaches 1,000 psi since their muscles get stronger with the increase in exercise. The maximum bite force in the patient without teeth is reduced to less than 50 psi, since they now must chew on the softer gums. The longer the patient is without teeth, the more the muscles atrophy and the less force they are able to generate. Patients wearing complete dentures for more than 15 years may have a maximum bite force of 5.6 psi, because the muscles decrease in strength and tone.
As a result of decreased bite force and the instability of the denture, chewing efficiency also is decreased with tooth loss. Within the same time frame, 90% of the food chewed with natural teeth fits through a no. 12 sieve; this is reduced to 58% in the patient wearing complete dentures. The 10-fold decrease in force and the 30% decrease in efficiency affects the patients ability to chew. A total of 29% of persons with dentures are able to eat only soft or mashed foods, while 50% avoid many foods, and 17% claim they eat more efficiently without the denture.
Removable partial dentures have one of the lowest patient acceptance rates in dentistry. A four-year Scandinavian study revealed that only 80% of patients who received partial dentures were wearing them after one year. The number further decreased to only 60% after four years. Reports of removable partial dentures indicate the health of the remaining teeth and surrounding gum tissues could deteriorate.
In a study that evaluated the need for repair of a tooth as the indicator of failure of the partial denture, the survival rate of conventional removable partial dentures was 40% after 5 years and 20% after 10 years. The patients wearing the partial dentures often exhibit greater mobility of the teeth, greater bacterial plaque retention, increased bleeding around the teeth, more incidence of decay and accelerated bone loss in the regions with no teeth. Therefore, alternative therapies which improve the oral conditions and maintain bone are often more desirable. The 5-year survival rates of partial dentures based upon tolerance and use of the dentures is approximately 60% when replacing molars and 80% for partials completely supported by teeth. This is reduced to 35% and 60% at 10 years respectively. In another study, few partial dentures survived more than 6 years. Although one out of 5 U.S. adults has had a removable denture of some type, 60% reported at least one problem with it.
So, Are Antiquated Full Dentures For You?
Todays denture treatments are no more effective than George Washington’s wooden teeth. If you have a choice to either keep your own teeth or if you must have them removed due to gum disease or decay please consider the above very carefully. The decisions that you make today may affect you for the rest of your life.
Dental implants preserve bone, preserve facial appearance, maintain function and help people feel younger and more alive. Dentures make people feel old. At Pinnacle Center Dental Implants and Periodontics our mission is to maintain the quality of life so that you can live and age with dignity and grace.
Experience the benefits of Dental Implants in Pittsburgh
